
It’s a wrap!
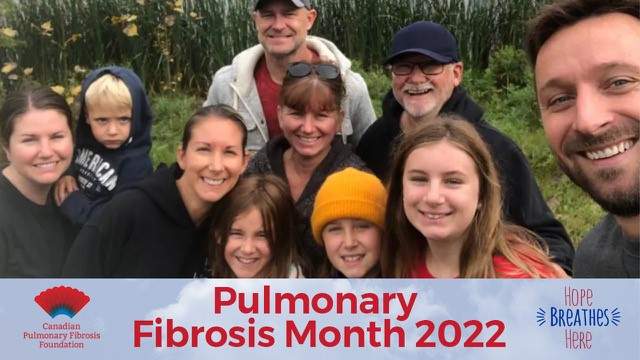
CPFFs 2022 Pulmonary Fibrosis Awareness Month campaign wrapped up at the end of September. And once again, our joint efforts have achieved great results. You’ll want to watch our CPFF 2022 Pulmonary Fibrosis Month Highlight Reel video today with detailed results and plenty of participant photos.
One of our goals was to collectively walk the 6,818 km across Canada in the CPFF Virtual Walk, Roll, Run. We surpassed our goal, walking 7,266 kms. Congratulations to everyone who participated and thank you to all those who pledged their support!
On the fundraising side, we raised $111,120! Quite an achievement in this time of economic uncertainty. Our supporters are devoted and our volunteers outstanding.
“We owe our successes to our donors, volunteers, sponsors, the people who arranged their own events and our staff and contributors who helped organize the campaign,” says Sharon Lee, CPFF Executive Director. “A special thank you goes to our experts who freely shared their knowledge in our series of webinars throughout the month.” If you missed them earlier, the educational webinars are all now available online to watch anytime.
Most of our donors and volunteers are, or are close to, people who live with pulmonary fibrosis or have passed away from the disease. Your dedication is wonderful and we would not achieve such success without you, says Lee.
Awareness Month greetings from elected officials have also been posted online. Plenty of landmarks were lit up in blue and red in recognition of Pulmonary Fibrosis Awareness Month and we garnered plenty of media and social media coverage, increasing awareness of PF across the country.
Please make the time to give yourself a hearty pat on the back and watch our CPFF 2022 Pulmonary Fibrosis Month Highlight Reel video soon.
Our PF resource library is loaded with helpful information
When you were first diagnosed with pulmonary fibrosis (PF), there’s a good chance you had never heard of this disease. The Pulmonary Fibrosis Resource Library on the new CPFF website is full of advice and insights from PF medical experts, patients, and caregivers to help you throughout your journey.
Added to the website last month, the resource library will help you better understand what PF is, the causes, symptoms, and what to expect as PF progresses. The topics covered range from diagnosis to treatment and care, including lung transplantation. There is information about support groups, COVID-19 and PF, participating in clinical trials and provincial health care resources. Just recently, the information on medication coverage in each province was updated.
If you’ve been recently diagnosed, or even if you’ve lived with the disease for a while, take some time to check out the PF resource library. Read through some of the information and watch a couple of the videos that may be of interest to you. You’ll soon understand that you are not alone and that others are facing the same challenges that you are facing. And, most importantly, there is help available.
We are adding new videos and other resources all the time that we find in the community, that may be helpful to our audiences. Please feel free to send us anything you’ve found helpful that may help others with PF. Submit links to other resources here: https://cpff.ca/contact/.
Learning about your disease is one of the foundations of self-advocacy. Visit the Pulmonary Fibrosis Resource Library today and begin your learning journey as you navigate life with pulmonary fibrosis.
CPFF community app

If you haven’t signed up for the free CPFF community app, think about doing so today. It’s not just for Awareness Month activities. It will keep you connected and informed all year long.
You can browse the app from your computer or download it from the app stores, Apple app store or the Google Play store.
Be sure to check out the CPFF event calendar on the app, or on our website for activities this month. You’ll find information about the National Patient Support Group meetings and the new National Caregiver Support Group meetings, both online. You’ll also find October sessions of the free online exercise program called Breathe Right.
If you know of any other free programs that would support people living with pulmonary fibrosis, please submit them to us for consideration here: https://cpff.ca/contact/.


Creating universal blood-type organs for transplant
Canadian Pulmonary Fibrosis Foundation (CPFF) audiences were fortunate to participate in a September 14 webinar featuring Dr. Marcelo Cypel, the senior author of a recent study into creating universal type O blood lungs. This research has the potential to significantly improve fairness in organ allocation and decrease mortality for patients on wait lists, especially for those with type O blood.
Currently, the blood types of people of Western European origin are about 50 per cent type O, about 35 to 40 per cent type A, with the remainder having type B or type AB blood. In other populations, the distribution may vary slightly; for instance, East Asian populations will have a higher proportion of people with type B blood.
“Along with other criteria, like lung size, blood type compatibility is one of the key requirements of lung transplantation,” says Dr. Cypel, Surgical Director of the Ajmera Transplant Centre at University Health Network (UHN) in Toronto. “And type O patients on the lung transplant waiting list experience a 20 per cent higher risk of dying compared to the other blood types.” This is because type O patients can only receive type O organs, but type A or B blood types can receive type O organs as well as their own blood type.
The “treatment” to convert type A, B, and AB lungs to O type lungs, involves removing a sugar, or antigen, which is only present in the surface of cells of A, B and AB blood-type cells, but not on O type cells. The antigen is removed by a pair of enzymes. The enzyme process was developed by University of British Columbia biochemist Dr. Stephen Withers and his team in 2019 to convert red blood cells for transfusions.
Dr. Cypel explained how his research study, which first involved tests at the cellular level using blood; then applied it to tissue, in this case aortas (the main artery that carries blood away from your heat to the rest of your body), and finally to actual pairs of lungs.
Human, type A, donor lungs, not suitable for transplantation, were put in the Ex Vivo Lung Perfusion (EVLP) system, which pumps nourishing fluids through the organs, enabling them to be warmed to body temperature, so that they can be repaired and improved before transplantation.
One lung was treated with the enzymes to clear the antigens from the surface of the organ, while the other lung, from the same donor, remained untreated. The enzymes removed more than 97 per cent of blood type A antigens within four hours.
“To test our hypothesis, we separated our study into two parts,” says Dr. Cypel. “The first part was to show the ability of enzymes to remove blood antigens from human lungs, without acute side effects and then we studied the effects of antigen depletion on preventing rejections.”
This was studied by bringing the lungs “back to life” or repurfusing them after treatment with the enzymes during EVLP, and preparing them as they would be before transplant. Results of this phase showed that the antigen removal prevented early antibody mediated rejection injuries. This type of rejection process occurs very rapidly, within 24 hours, and without intervention can be deadly, says Dr. Cypel.
Right now, the UHN team is studying longer-term, post-transplant responses, since it is likely that the antigens will regenerate within the organs. And, because animals have different blood types, testing cannot be done on animals before it is investigated in humans.
Dr. Cypel anticipates that the first of these treated lungs will be transplanted within a year’s time, into an informed and consenting patient on the transplant waiting list. Most likely into a recipient with O-type blood, with very low type-A antigens.
We all look forward to successful outcomes in people, offering new hope to those awaiting a lung transplant.
Read more about this research.
Watch a related presentation about IPF treatments, including lung transplantations, in the 2021 CPFF video “Therapies for IPF – from pills to lung transplantation,” featuring Dr. Shane Shapera and Dr. Shaf Keshavjee, both of UHN.
Genetics and interstitial lung disease
There is a lot of exciting research being done on genetics and interstitial lung disease (ILD), which may lead to useful tools to help patients and their family members, says Dr. Amanda Grant-Orser in her September 20 webinar for the Canadian Pulmonary Fibrosis Foundation (CPFF).
Dr. Grant-Orser, along with Dr. Kerri Johannson, both respirologists at the ILD Program at the University of Calgary, discussed genetics and ILD and Dr. Grant-Orser’s recent study published in the Annals of American Thoracic Society on the perceptions of genetic testing of ILD patients and their first-degree relatives. (First-degree relatives include parents, siblings and children.) Dr. Grant-Orser’s research was part of her work as a 2020 CPFF Robert Davidson Fellow. And participants in her study included those who responded to her survey, which was promoted by CPFF.
Beginning with basics, Dr. Grant-Orser discussed how genetics refers to DNA analysis and gene variants and single-nucleotide polymorphisms (or SNPs, pronounced snips). A SNP is a genomic variant at a single base position in the DNA. Scientists study if and how SNPs in a genome influence health, disease, drug response and other traits.
She also mentioned telomeres – the protective caps at the end of each strand of DNA. She likened them to the plastic ends on shoelaces and noted that as cells divide the telomeres get shorter, but DNA remains protected. Eventually the telomeres become too short and the cells stop functioning properly. ILD patients are more likely to have short telomeres than the general population, and have a worse prognosis, regardless of the type of ILD they have.
An identified SNP, called MUC5B, is present in up to 40 per cent of those patients with IPF. Could it be an indicator that could be used in a prediction model for IPF? Could it become a screening tool?
At present, genetics alone do not explain most causes of ILD and most patients will not have a genetic cause. Even in families with a strong history, a causative gene may not be found. So why should we study genetics and ILD?
“Genetics may enable us to detect disease earlier,” says Dr. Grant-Orser. “And they may help us to predict outcomes and screen family members.” All of which may help us to intervene to prevent progression to ILD.
Another possible “predictor” of ILDs are interstitial lung abnormalities (ILAs), which is not a genetic test. In general, CT scans are being done much more often. And incidental (ILAs) are increasingly being found on CT scans. While ILAs are not a “disease” by themselves, they may indicate a need for follow-up. In the “normal” population, about five to 10 per cent will have ILAs and of those people, 20 to 40 per cent will develop an ILD.
Dr. Grant-Orser proceeds to ask and answer several questions : “Can we use genetics to identify high risk people? If we identify high risk people early, can we prevent irreversible fibrosis? Can we better predict outcomes? What treatment should we use? What is the role of preventative health measure like smoking cessation, vaccines, etc.?
What if you have a family history of ILDs? In general, patients with a family history of ILD had a worse prognosis. In patients with a family history of two or more relatives with ILD, 20 to 25 per cent of them have identified genes and 14 to 31 per cent of first-degree “at risk” relatives will show a change in CT scans.
What does this mean in practical terms for family members of ILD patients? Let your doctor know family members have ILDs. Your physician can then listen for crackles in your lungs. Do not ignore symptoms like a persistent cough. While there are no preventative treatments, try to reduce your risk factors like smoking or occupational exposures. And keep up with your vaccines for respiratory illnesses.
And what about genetic testing? There are several considerations. Will the tests be likely to identify anything useful? Is there access to genetic testing and genetic counselling? These are not widely available in Canada. And, is there access to medications for treatment? Anti-fibrotic medications are available and covered in almost every part of the country.
Most importantly, Dr. Grant-Orser’s recent study evaluated what patients and their first-degree relatives thought about genetic testing. An online survey, distributed by CPFF, among others, garnered 188 respondents and 20 people took part in online focus groups to delve more deeply into their perceptions.
Sixty-seven per cent of survey respondents said they would be interested in genetic testing to look for genes associated with ILD. Fifty percent did not know if there was a genetic cause to their own or a family member’s ILD. And 55 per cent worried that other family members could be affected by ILD.
Asked about how genetic testing could affect certain factors, 45 per cent were concerned about access to life, disability and travel insurance; 37 per cent were concerned about personal stress and anxiety; 52 per cent thought testing could affect their children’s and other family members’ health and 20 per cent thought testing may affect their health behaviors.
The focus groups centred on four themes around genetic testing: improving ILD disease knowledge and resource access; the role of genetics in ILD; testing concerns such as insurance, disclosure and family concerns and the use of genetic testing information, such as identifying those at risk and treatment input.
If you are eligible for genetic testing, should you get tested? Dr. Grant-Orser had these tips and considerations:
- Discuss it with your respirologist
- Undergo genetic counselling beforehand
- May help explain why you have ILD
- May help understand how/if your disease will progress
- May help doctors look for other things: blood or liver problems
- Help us better understand ILD and contribute to research
In closing her presentation, Dr. Grant-Orser sent a special thank you to all of the participants of the survey and the focus groups!
Editor’ Note: An EU-IPFF webinar on genetics and pulmonary fibrosis with Dr. Richard Allen in the UK is also available online.
Everything you need to know to start your advanced care plan
As the worst of the pandemic subsides, more Canadians than ever are talking about Advance Care Planning (ACP), although only 17 per cent actually have a written advanced care plan (ACP), according to Karine Diedrich, Director, Operations and Engagement at the Canadian Hospice Palliative Care Association (CHPCA). Diedrich shared “The what, who, when and how of ACP,” in her September 15 webinar for CPFF.
ACP is not about creating a laundry list of treatments you may want and those you do not want,” says Diedrich. “It’s thinking about what is important to you and using that information to inform the health decisions you will make throughout your life.”
She related anecdotes of one man who accepted any treatment, as long as he could still watch football on TV at home and eat chocolate ice cream. Another woman wanted to attend the upcoming wedding of her granddaughter and wanted any treatment that might prolong her life until that day.
Advance care planning is a process of reflection and communication, says Diedrich. A time for you to reflect on your values and wishes, and to let people know what kind of health and personal care you would want in the future if you were unable to speak for yourself.
ACP does not need to be complicated or require professional services, although some people may wish to engage a lawyer. There are plenty of resources online to help you with the process. Visit www.advancecareplanning.ca for tools, resources and workbooks.
It may help to think of advance care planning as part of your “life” plan. Just as you plan for financial goals, buy insurance, and write a will for your estate, you should have a plan for your health care. Like these other plans, your ACP will change as your life changes: when you get married, have children, retire, or are diagnosed with a chronic illness or undergo major surgery.
Having an advanced care plan is also helpful for health care professionals. In a moment of crisis, ACP helps everyone; the patient, family members and health care professionals are better prepared, and hopefully in agreement, since this is not the first time that everyone involved has thought of this possibility.
During her webinar, Diedrich described the five steps of advanced care planning.
Step 1: Think
What makes life worth living? That may depend on where you are in life and your thoughts may change over time.
If you are a healthy adult, think about:
- Any specific wishes you already have
- How to ensure your wishes are honoured
- Who you would choose to make decisions for you.
If you are older and coping with a serious illness or frailty, think about:
- What do quality of life and comfort mean to you?
- What are you willing to go through for the possibility of more time?
- How would you like your dying experience to be when the time comes?
- Have you talked enough with those who matter to you and your health care professionals about your wishes?
Step 2: Learn
To make informed decisions, talk to your health care professionals about your health. You need to know the benefits and drawbacks of all your care options.
Step 3: Decide
When you need health care, it’s up to you to decide whether or not you want the treatment, and then either give or refuse consent. If you are unable to decide for yourself you need someone to decide and speak for you. That person is your substitute decision maker
When choosing a substitute decision maker (SDM), try to choose someone who:
- Is a capable adult
- Will honour your wishes even if they are different from their own — this is their legal role
- Is calm in a crisis
- Is able to handle conflict or disagreement (e.g. family members do not agree with your decision or your substitute decision maker does not agree with the options provided by your health-care professional)
- Is accessible and able to commit the time that might be required.
If you do not have a designated SDM, or your SDM is not available, your health care professionals will turn to other people in your life in the order they are listed in your province or territory. Check Section 3, “Regional Summaries” in this workbook for more information about substitute decision makers in your province or territory.
Step 4: Talk
- Share your thoughts about what is important to you and what your goals are with people who matter to you.
- Talk about your biggest fears and worries about your future health.
- Discuss who will speak for you and how you want that person(s) supported.
- Remember to talk to your health care professionals. By keeping them informed you are more likely to get the kind of care you want. Tell them your wishes for your current care, who your substitute decision maker is and any other information they need to follow your wishes. Be sure they know what living well means to you and what treatments you are willing to undergo for the possibility of more time.
Step 5: Record
There is no legal requirement to write down or record your wishes, but recording can help:
- you remember what you thought and said
- your substitute decision maker remember the details of the discussion
- the people involved in your care because it provides evidence of your wishes if there is disagreement about your care.
Consider recording your wishes and what matters most to you in a health care planning document or some other form. You can find some at www.advancecareplanning.ca.
The record should include:
- documentation or voice/video recording of your values, goals and wishes
- a list of your potential substitute decision maker(s)
- any legal documents, such as documents that name your substitute decision maker(s)
Finally, although it is not an advance care planning step, take the time to review your ACP on a regular basis, or whenever there’s a change in your life or health.
Can a digital tool help you better manage your own care?
Are you and your care partner struggling with managing appointments, medications and even oxygen supply? Are you tired of reproducing your medical history over and over? Audrey Bond, Founder and CEO of Vaultt, a digital health app, delivered a CPFF webinar on September 13, sharing possible solutions to these and several other health care challenges.
Bond’s outlook is unique in that she has been a caregiver for more than 20 years and has been an entrepreneur for more than 25 years. Her mother became paraplegic when Audrey was 12 and her father died recently after living with dementia. In addition, she lives with neurological issues of her own.
With millions of people now living with a chronic disease, industry and health care providers have responded with thousands of digital tools to help manage ongoing care. This has only increased as people became more comfortable with telehealth and digital health care delivery during the pandemic. However, most of the tools are built with the institution or provider as the primary client, not the patient or caregiver, says Bond.
“As a caregiver, I was stressed trying to manage my parents vital personal and health information, appointments, prescriptions and everything else involved in their care,” says Bond. “And, I needed to share and coordinate everything with my brother. Documents for taxes, insurance and medical requisitions were stored in different places and not shareable. There had to be a better way to organize all of this.”
Not finding what she needed in the marketplace, she founded Vaultt. “Our mission is to help as many patients, families and caregivers as possible stay organized and connected, alleviate stress and give people back control of their data by building an end-to-end encrypted organizational platform for families and caregivers.”
While Bond is no doubt promoting her own product Vaultt, and her approach, “built for patients and caregivers, by patients and caregivers,” she did make some very valid points if you are considering using a health management app.
With Vaultt, your data is “owned” by you and only you can designate access to the information, which can be revoked by you at any time. And your information will never be shared or sold. “And if the app is free, you are the product and your data is being mined to target you to other organizations and advertisers,” says Bond.
As the name implies, Vaultt is more secure than most mobile financial apps, declares Bond. This is of particular concern since individual health information is very private and 62 per cent of data breaches were in the health care industry in 2021.
Right now, Vaultt is only available on the Apple store, but by year-end it should be available for Android phones as well. And, integration with wearables (like watches that track vital signs) will be added for tracking. In 2023, Vaultt intends to add integration with electronic health records and secure messaging between patients and health care providers. For now, you can email information to your doctor from your app.
The Vaultt app is $5.99 per month for the full platform with a free 14-day trial available to try it out. Features allow you to track, store, secure and share your health information and other related documents. You can find out more at https://www.vaultt.com/.
Check out Audrey Bond’s presentation for more information about her product and things to consider when deciding on a health care app, including data ownership, security, features and value.
T-shirts available from John Dennis

John Dennis, a pulmonary fibrosis patient and lung transplant recipient, rode his electric bicycle around PEI this past June, raising funds and awareness for PF. He now has his own t-shirt for sale. If you are interesting in purchasing one, or want to know more, contact John directly at [email protected].