
Palliative Care
Comfort and dignity until the end.
Palliative care addresses pain and symptom management and provides social, psychological, emotional and spiritual support, as well as providing support to caregivers and family members.
Support for those living with a life-limiting illness

Palliative care isn’t just about end-of-life — it’s about living well. For people with a serious or incurable illness like pulmonary fibrosis, palliative care focuses on improving quality of life every single day. It’s about paying close attention to the symptoms that make life harder — breathlessness, fatigue, pain, sleep problems, anxiety — and finding ways to ease them so you can focus on the things that matter most to you. Good palliative care is a team approach, bringing together doctors, nurses, respiratory therapists, physiotherapists, occupational therapists, and counselors, all working with you and your loved ones. It supports not just your health, but your circle of family and friends too, helping everyone live as well as possible while navigating life with PF.
Most individuals living with pulmonary fibrosis would benefit from early access to palliative care according to Dr. Doris Barwich, Medical Director, BC Centre for Palliative Care and Dr. Shalini Nayar, of Surrey Memorial Hospital and a specialist in both respiratory medicine and palliative care.
Palliative care is not only for end-of life, but is a specialized form of healthcare for individuals and families who are living with a life-limiting illness that is usually at an advanced stage. The goal of palliative care is to provide comfort and dignity for the person living with the illness, as well as the best quality of life for both the individual and their family.
“Several studies on hospice palliative care offered to people with IPF indicate that there is a great need for early integrative palliative care with advance care plans to improve the end-of-life care.” — Dr. Doris Barwich, Medical Director, BC Centre for Palliative Care
Gain an Understanding of Disease Progression
In the last year of life, what is most important to individuals is having a realistic understanding of their expected symptoms, quality of life and disease progression. Palliative care supports can prepare the person experiencing the symptoms and their caregivers. A palliative care team can help with advance care planning (ACP), including identification of goals of care and an action plan for a crisis, which reduces stress and anxiety and often the number of visits to the emergency department.
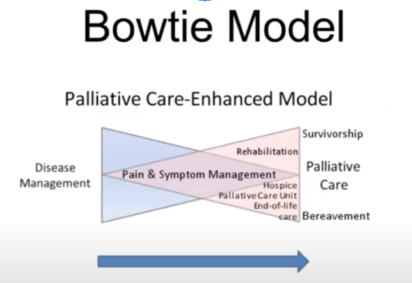
Where Disease Management Intersects with Palliative Care
Dr. Shalini of Nayar of Surrey Memorial Hospital and a specialist in both respiratory medicine and palliative care shares the Bowtie Model of care in a CPFF hosted webinar. This is where disease management intersects with palliative care. Pain and symptom management fall within both categories, with rehab and end-of-life care added to the palliative side of the bow. Watch webinar.
1. The terminal illness trajectory (usually cancer deaths) is generally predictable with a short course of a few years with more rapidly progressive decline in the last few months of life.
2. The organ failure trajectory is a longer course of slow decline with intermittent acute, life-threatening episodes and then a seemingly “sudden” death. Often this would occur over a period of two to five years. This would be common, for example, with lung or heart failure.
3. The frailty trajectory is a long course of slow unpredictable deterioration with the ability to self-care decreasing over time, maybe even over as much as six to eight years. This would be consistent with the frail elderly and dementia.
Dr. Shalini shares that most approaches to palliative care follow those facing the terminal illness trajectory, but it is clear that those facing the organ failure or frailty trajectory could also benefit from palliative care.
Who Might Benefit from a Palliative Care Approach?
Medical professionals evaluate the fit for palliative care for those living with interstitial lung disease (ILDs) with these questions:
- Does the patient want or need supportive care?
- Would the healthcare team, or family members, be surprised if this patient were to die in the next year?
- Has the patient had more than two admissions to ICU for ventilation?
- Are they experiencing increased breathlessness?
- Have test results shown substantial reduction in lung function?
- Clinical indicators can include: a DLCO (diffusing ability of the lungs) less than 40 percent; oxygen levels less than 88 per cent during the six-minute walk, increased scarring on CT scans, and a decrease of more than 10 percent of FVC (forced vital capacity) over a set period of time.
Patients are waiting for their doctor to begin discussions
Patients are generally aware and state their preferences, but they are often waiting for health care professionals to begin discussions, especially about end-of-life care. It is worth noting that caregivers are often inaccurate about a patient’s quality of life.
Health care teams can be reluctant to suggest palliative care
The health care team can also be reluctant to suggest palliative care for many reasons, such as: unrealistic expectations of recovery; lack of awareness of options when a recovery is no longer possible; difficulty withdrawing or withholding care; a lack of experience or discomfort in breaking bad news; a lack of time, privacy or too many interruptions for discussions; and personal and professional experiences with illness and death.
Misconceptions around medications
There are medications that can ease pain and anxiety for ILD patients. Again, there are still misconceptions, both by patients and health care providers. The judicious use of opioids for pain management in pulmonary patients is safe and does not suppress respiration. Opioids can also ease breathlessness. Benzodiazepines can help relieve anxiety, which can be brought on by breathlessness and general uncertainty and fears.
Plan for the Future
Advance care planning can help to relieve anxiety for both people living with pulmonary fibrosis and their families. Part of that plan should be the preferred place of death. Home palliative care is an option. Select your substitute decision maker to speak for you when you are no longer able, and make sure they understand what’s important to you. See 5 steps to creating an advance care plan.

More on Palliative Care

Palliative Care and Advance Care Planning – Dr. Tim Heibert
In this video, Dr. Heibert, a palliative care specialist, shares powerful insights on how to plan ahead and communicate your healthcare wishes clearly.

Palliative Care for ILD: Exploring Cannabis – Dr Rebecca Colman
Tune in as Dr. Rebecca Colman explains palliative care and symptom management in interstitial lung disease (ILD) and discusses the role of cannabis to alleviate symptoms.
Advance Care Planning – Karine Diedrich
Learn about advance care planning, a process of reflection and communication. It is a time for you to reflect on your values and wishes, and to let people know what kind of health and personal care you would want in the future if you were unable to speak for yourself.
Manitoba Palliative Care
Learn about palliative care for people living with pulmonary fibrosis in Manitoba.

Living and Dying Well in Alberta
Learn about palliative care for people living with pulmonary fibrosis in Alberta.

Palliative Care in Canada
Laurel Gillespie, CEO of the Canadian Hospice Palliative Care Association (CHPCA) discusses palliative care in Canada.
Read More…
Advance Care Planning in Your Province
Learn about Advance Care Planning in your province.
Hospice Palliative Care in Canada
Get education and resources from the Canadian Hospice Palliative Care Association.
Access Palliative Care in Your Province
Learn how to access palliative care in your province.